We're creating better, patient-centered resources to promote shared decision-making.
What is a decision support tool (DST)?
You may have already used one. DSTs can include brochures, audiovisual materials, educational sessions, interactive websites or counseling sessions, used separately or in combination. These media allow a patient to vocalize their needs, goals and expectation when discussing their care.
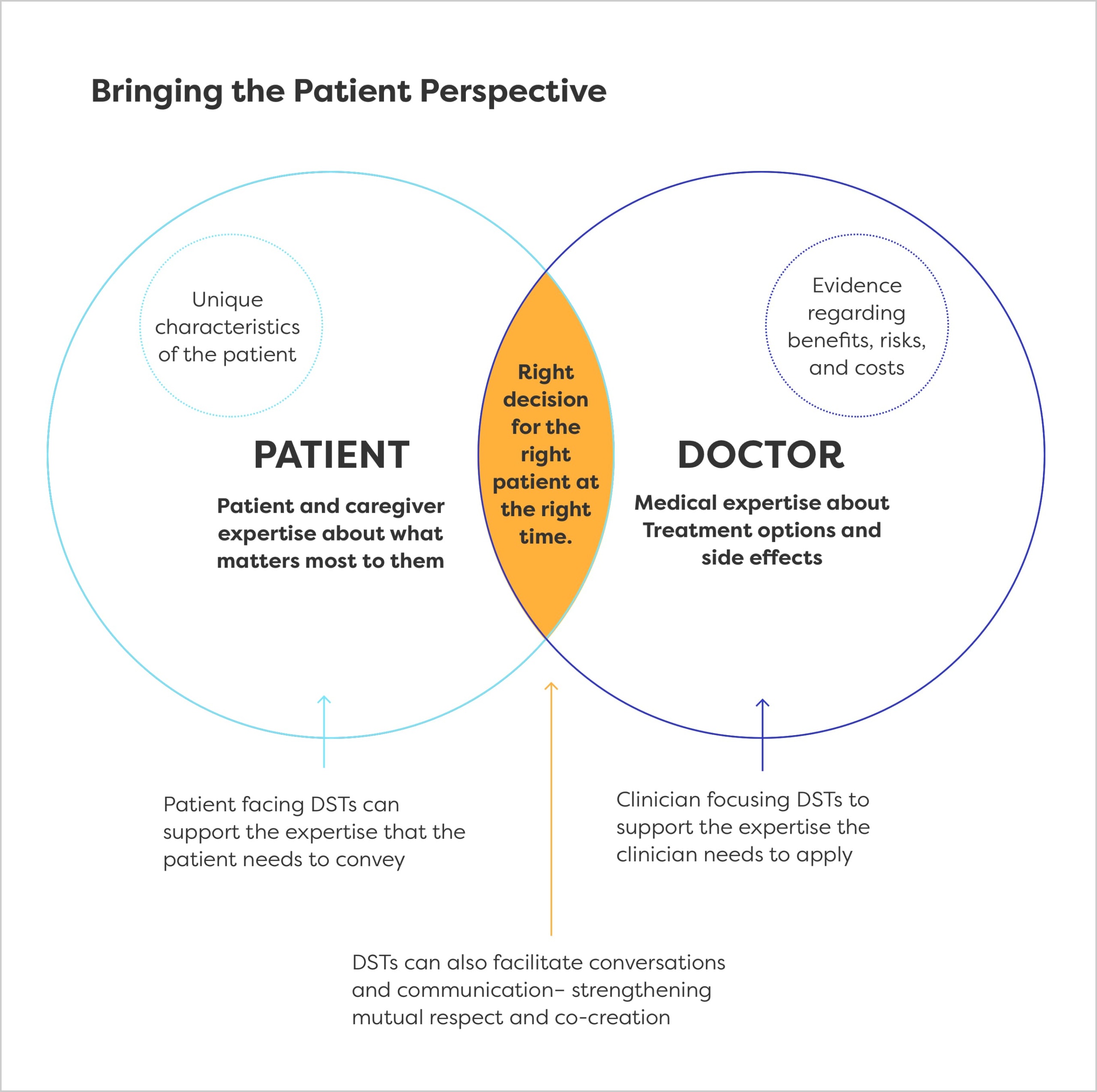
DSTs do not replace health care providers and are intended to facilitate a shared decision-making conversation. They complement the patient-provider interaction and align two very important sources of knowledge to enable the delivery of co-created care that integrates the medical evidence with personal preference.
Decision Support Tools: Bringing the Patient Perspective
Decision support tools (DSTs) help patients and their health care providers participate in decision making about their health care options. They utilize structured guidance to encourage open, honest communication about the likely benefits and harms for treatment options as well as provideopportunities for patients to identify and articulate their values and preferences. Effective use of DSTs is critical to shared decision-making and coordinated care planning. These tools should be available at every important decision point throughout the care continuum.
Figure 1
Decision support tools have the ability to be incorporated atmultiple points along a patients care journey and in a variety of formats. To better understand the when and where of these uses, we created four domains that DST can be attributed to:
Targeted (patient-facing)
Self-led materials to inform decision making. These may be given to the patient by the provider, but often are found by the patient independently or via disease advocacy group or patient navigator.
Targeted (clinician-facing)
Used by clinician to guide treatment/care decisions, tool is not designed to be used by, or shared with, patients or caregivers.
Collaborative (patient-initiated)
Used by patient or caregiver during clinical interaction to facilitate SDM or care planning conversation
Collaborative (clinician-initiated)
Used by provider during clinical interaction to facilitate SDM or care planning conversation
Although we were able to bucket many of the available DSTs into types that supported patient-clinical decision making conversations, DSTs may not be “patient-centered.” To address this this design gap we proposed a novel project to introduce the concept of patient-centric review criteria to an existing evaluative infrastructure.
The Project
Patient Advocate Foundation and National Patient Advocate Foundation are engaged in an initiative to create a comprehensive set of design and implementation standards, along with supporting resources, that will serve as the foundation for a new person-centered accreditation program for decision support tools in cancer and cardiovascular disease.
Previous Work
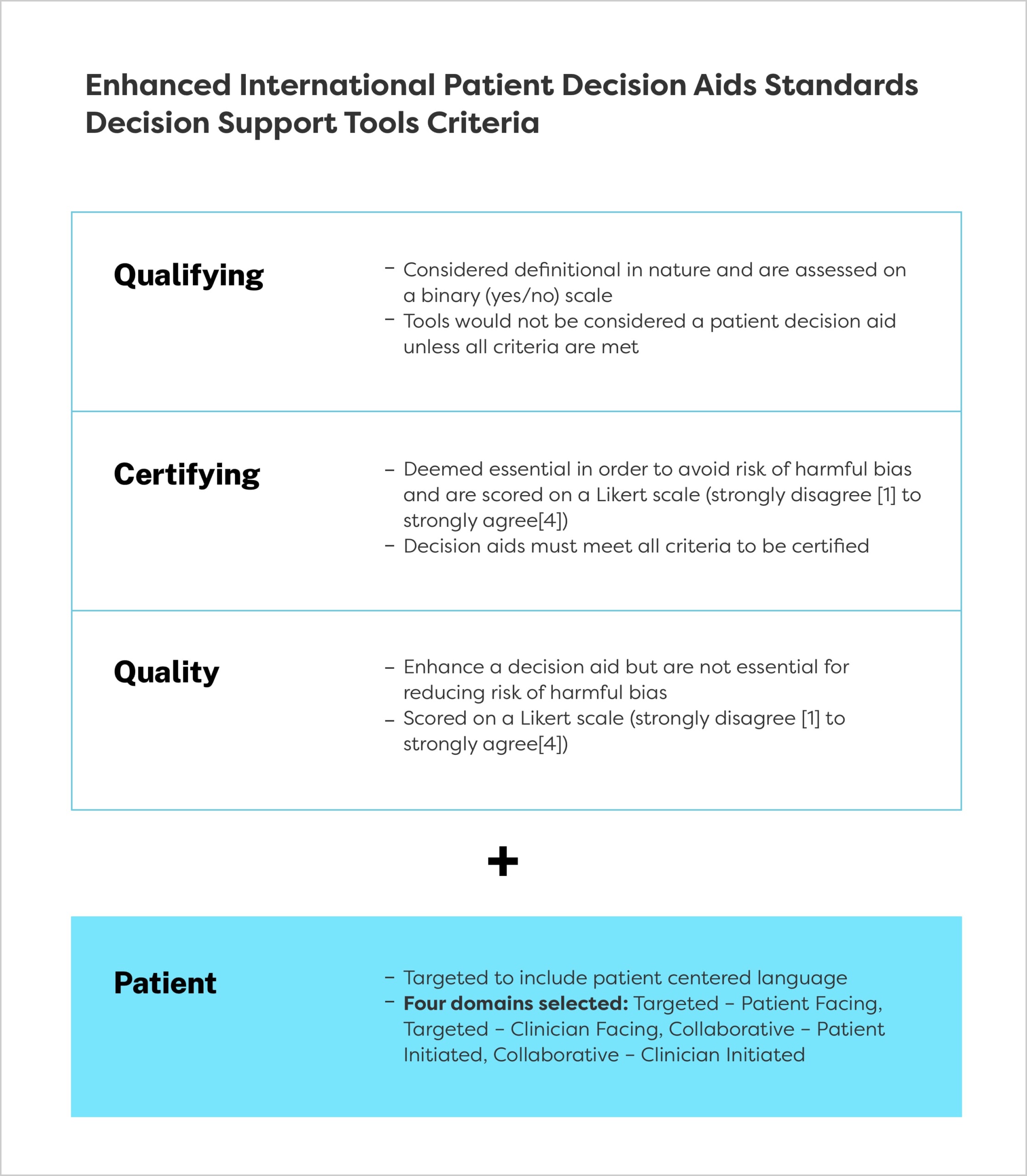
This initiative builds on a substantial body of effort by the International Patient Decision Aids Standards (IPDAS) Collaboration, an international group of researchers, practitioners and stakeholders interested in the design and use of patient decision aids. The group, recognizing that certification of DSTs is becoming a priority for health systems, undertook the challenge of identifying a minimal set of standards that can be used to certify the quality of a patient decision aid. The end results were 44 criteria, organized into three categories. The goal of our current project is to enhance these criteria to reflect the patient experience and point of view more fully and accurately (Figure 2).
Figure 2: Enhanced IPDAS DST criteria
PAF developed patient-centered criteria to address gaps in the existing IPDAS criteria to provide a stronger foundation for evaluating patient-facing or collaborative patient-initiating DSTs.
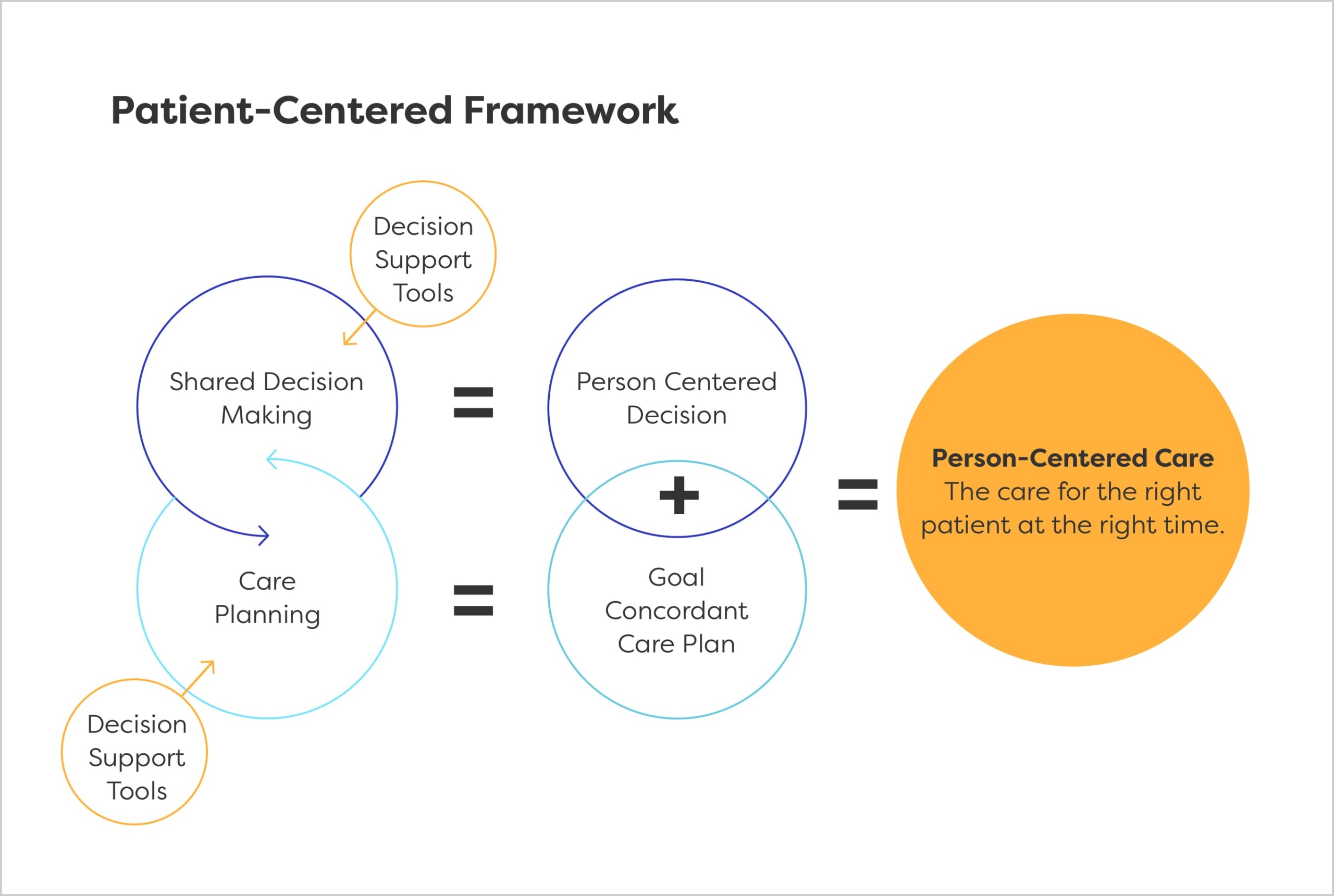
Shared decision making and care planning are the foundations on which co-created person-centered care can be delivered. There are three essential components that shape the patient experience. This project seeks to ensure that all of these critical components are embodied in DSTs and understood by the patients who use them.
Respect
Seeing and treating each person as an individual. Not making assumptions or judgements
Listening
Genuine, two-way discussions, based on active listening
Personal Connection
Acknowledging a relationship on a personal level between the patient and provider.
Our goals are to:
Create an infrastructure that can be used to evaluate existing tools and provide recommendations for improving patient centeredness
Identify gaps and develop criteria that address patient values and priorities
Disseminate best practices to guide the development of future tools using enhanced criteria
Work to Date
In the first two phases of this project, we have:
Completed a landscape analysis of all specific criteria related to DSTs
Analyzed specific overlaps/gaps between current criteria and those we are proposing to address person-centered dimensions
Developed specific criteria for each dimension
Conducted an external review of the feasibility of applying new and existing criteria to specific DSTs.
Held a summit to rank new and existing criteria and discuss potential scoring approaches
To create this patient-centered set of criteria, the PAF/NPAF team reviewed the 44 criteria and selected a subset for inclusion into a that could be used to evaluate DSTs.
Figure 3: Patient-Centered Framework
These included four of the six qualifying criteria, three of the ten certifying criteria and nine of the twenty-eight quality criteria. We modified the language of six criteria to make them more patient focused and developed 11 new patient-centered criteria. Some of these were incorporated in the existing IPDAS categories, the others we added to a new, fourth category.
Expert Testing and Review
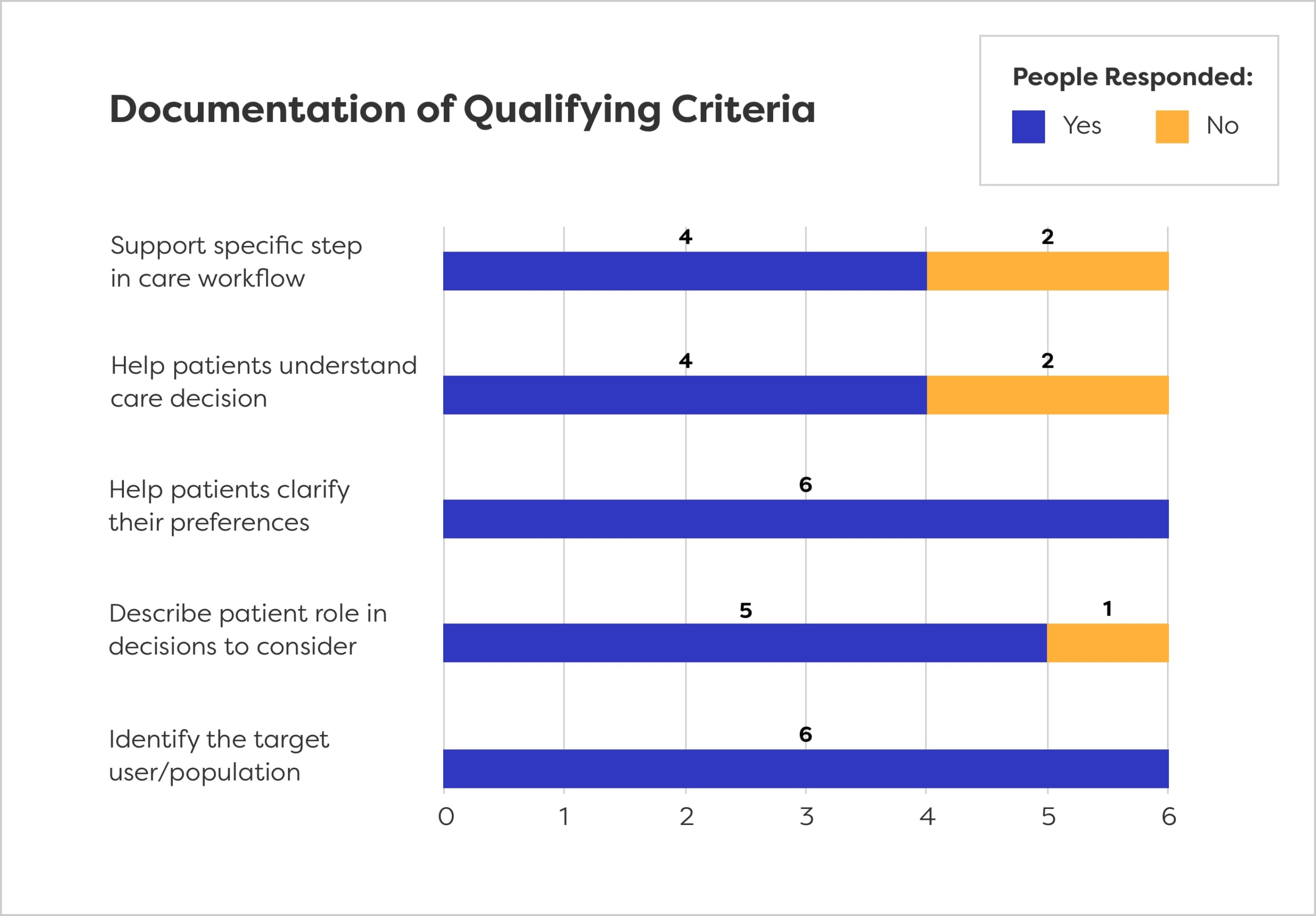
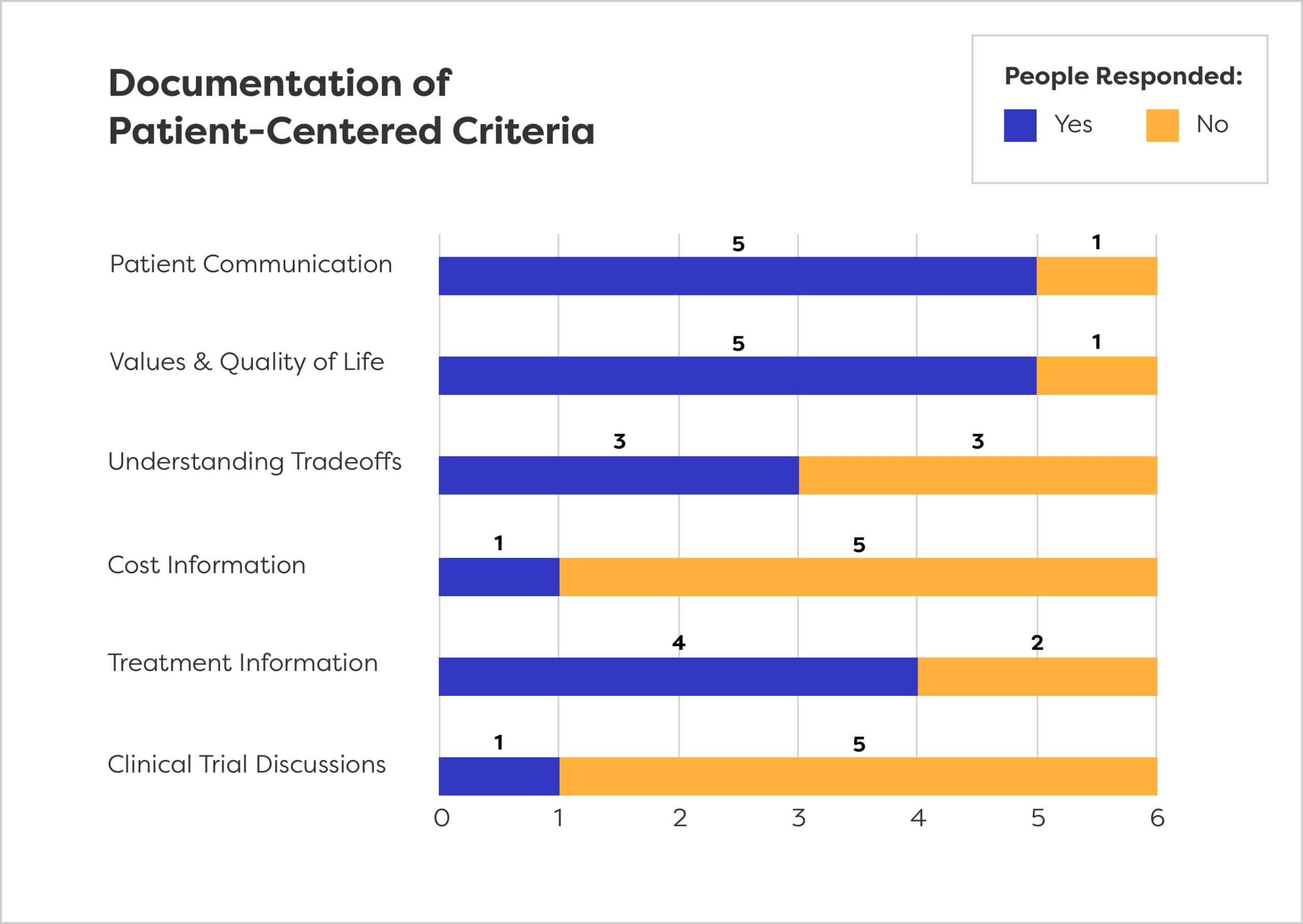
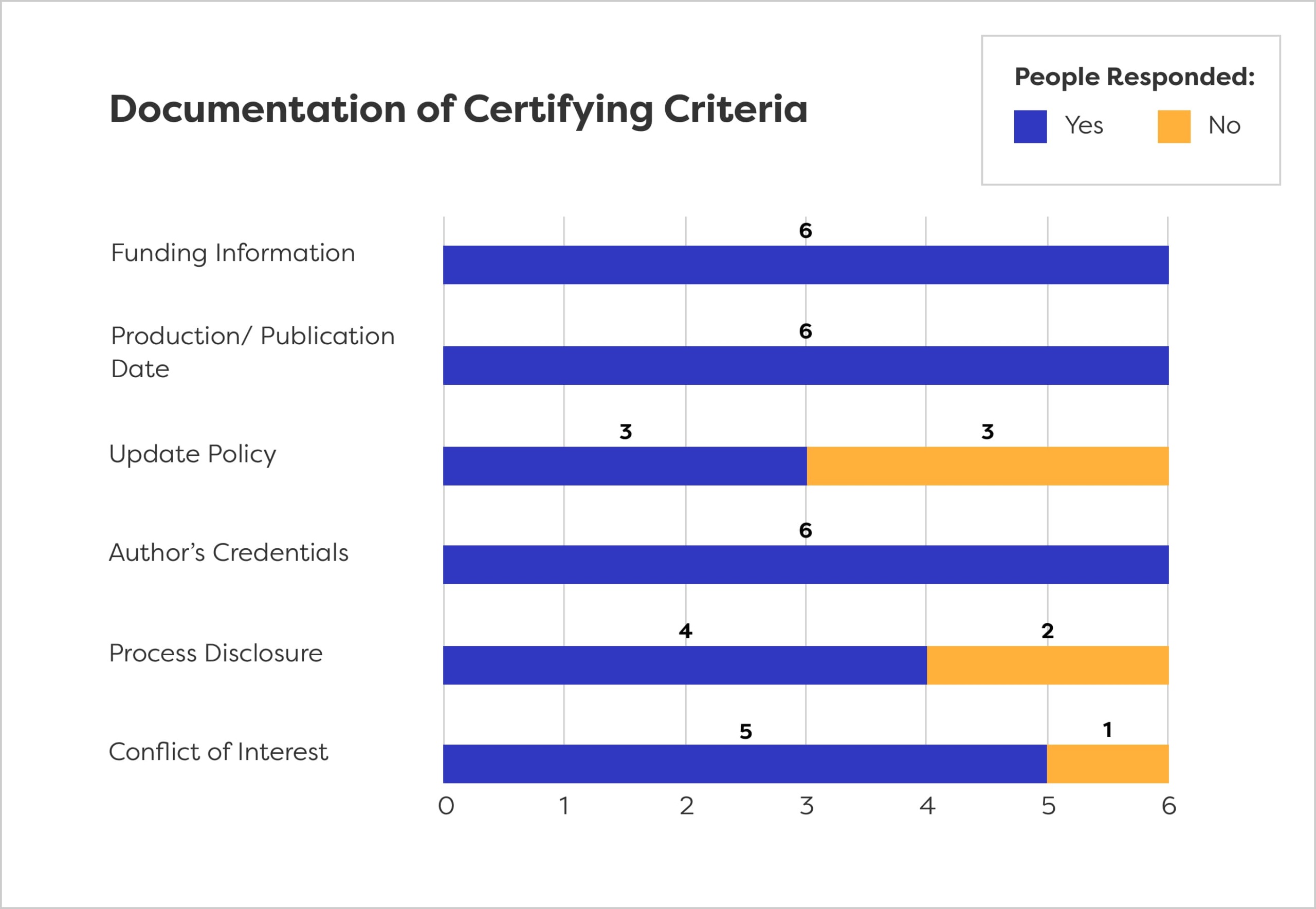
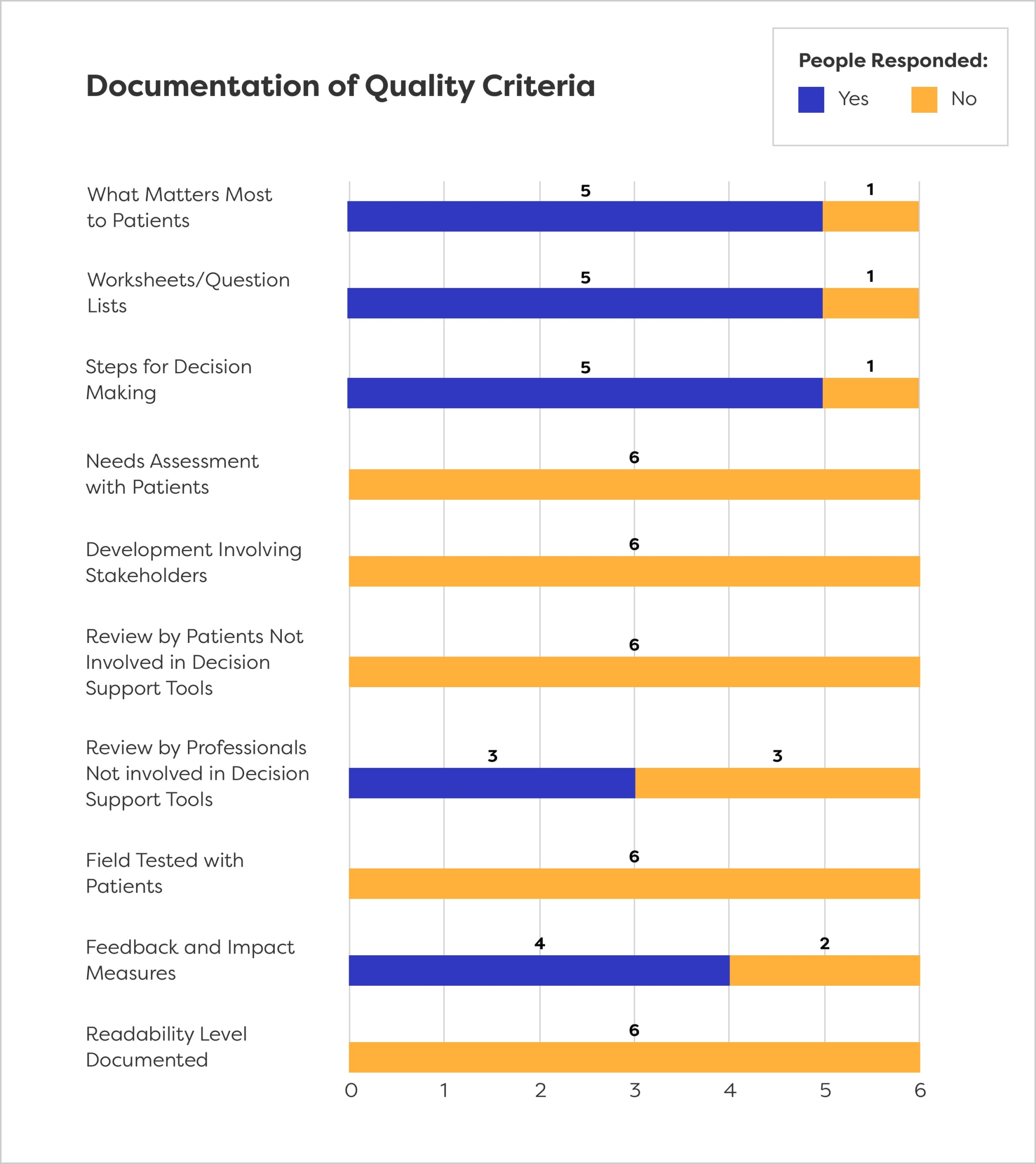
PAF/NPAF recruited a panel of experts to evaluate our 27 criteria using one of our domains–targeted patient facing tools with no clinical options. We ask six experts to review the selected tool using a binary formula to determine if they could locate all the criteria in the specific tool. The results are shown below (Figure 4).
Figure 4: Criteria Documentation
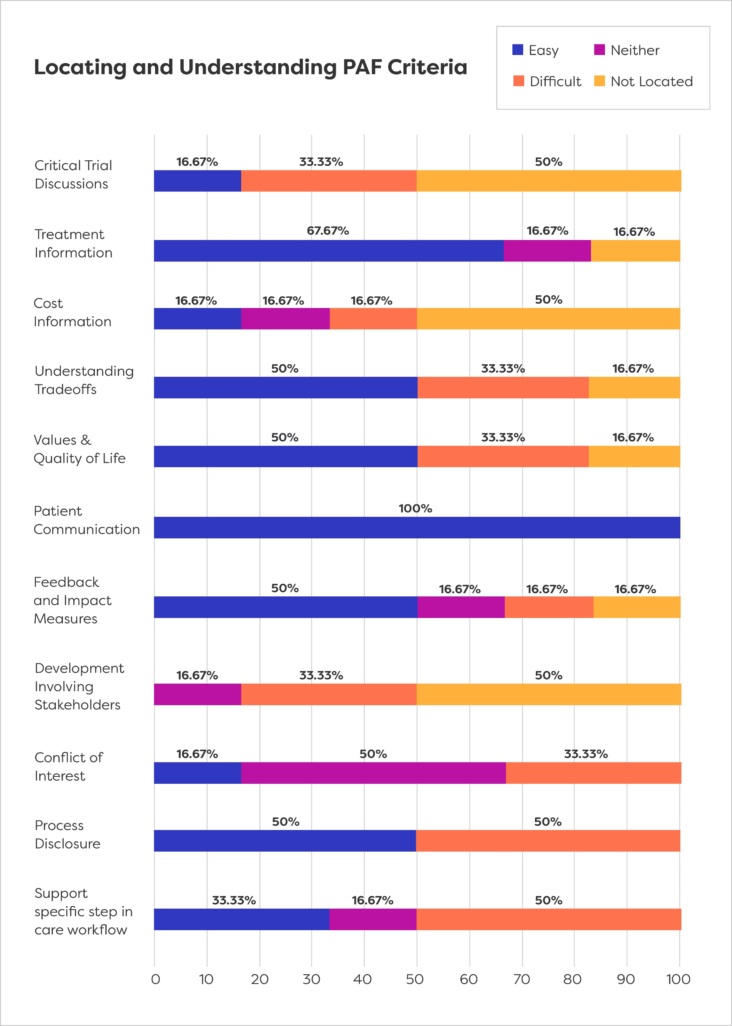
Figure 5: Locating and Understanding PAF Criteria
We also asked reviewers to describe their on-line experience. Based on the feedback we received, locating and interpreting the newly created criteria proved to be one of the biggest challenges faced by our team of 6 reviewers.
In addition, presentation of the criteria was subjective – many reviewers felt that binary responses such as Y/N were difficult use – if they had a range of options to apply (none, a little, some, a lot) answering in the affirmative would have been easier (Table 1).
Table 1: Appropriateness of Binary Response Metrics for PAF Criteria
Binary Response
Process disclosure
5/6
Conflict of interest
5/6
Feedback and impact measures
5/6
Clinical trial discussions
6/6
None of the criteria were universally listed as missing and, in most instances, more than half of the reviewers found what they considered to be language meeting these criteria. This leads us to believe that it was not lack of available information meeting the criteria requirements, but more a restriction of either time to search for this information in the supporting documentation, or interpretation of the material contained in the DST.
The Stakeholder Summit
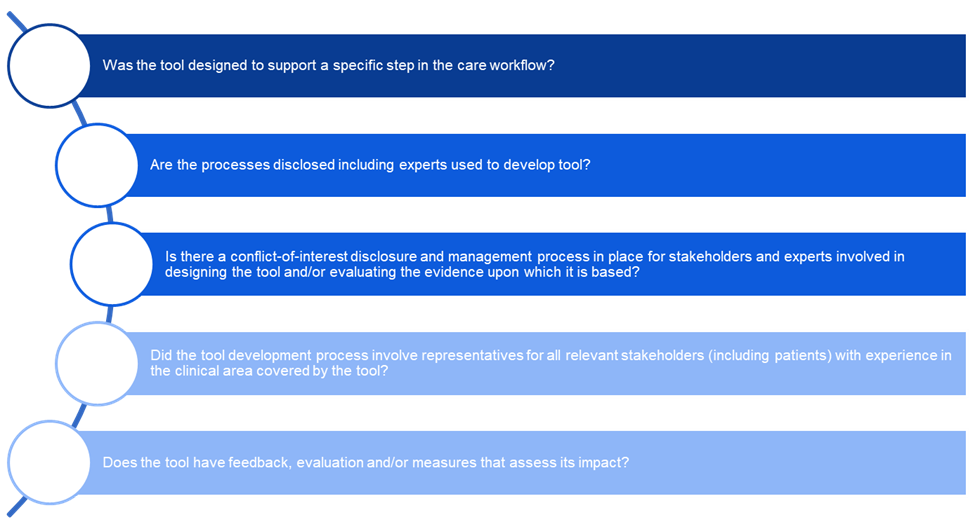
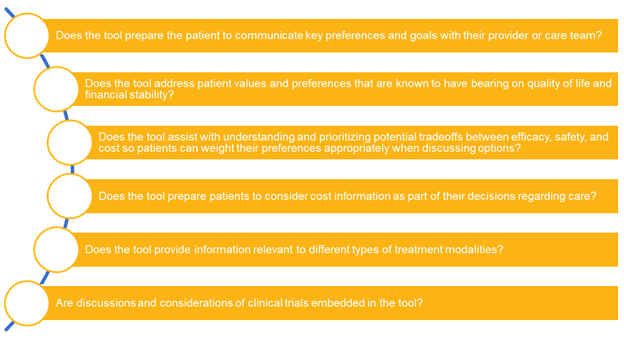
The next involved assembling a panel of experts, including patients and advocates, to rank or prioritize the eleven PAF-created criteria (Figure 6), to identify potential responses and scoring metrics, and to touch on language and determine gaps and items for removal.
Blue shades: Original IPDAS criteria
Yellow shades: Newly developed patient domain
The summit participants were divided into two focus groups. Group I was charged with ranking the 11 items in terms of their importance (Table 2).
Table 2: PAF Criteria Ranked by Level of Importance
*Italicized items correspond to criteria selected by PAF for our patient centered criteria list
Rank
PAF Criteria
1*
Does the tool assist with understanding and prioritizing potential tradeoffs between efficacy, safety, and cost so patients can weight their preferences appropriately when discussing options?
2*
Does the tool address patient values and preferences that are known to have bearing on quality of life and financial stability?
3*
Does the tool prepare the patient to communicate key preferences and goals with their provider or care team?
4
Does the tool provide information relevant to different types of treatment modalities?
5
Does the tool prepare patients to consider cost information as part of their decisions regarding care?
6
Does the tool have feedback, evaluation and/or measures that assess its impact?
7
Are discussions and considerations of clinical trials embedded in the tool?
8
Is there a conflict-of-interest disclosure and management process in place for stakeholders and experts involved in designing the tool and/or evaluating the evidence upon which it is based?
9
Did the tool development process involve representatives for all relevant stakeholders (including patients) with experience in the clinical area covered by the tool?
10
Was the tool designed to support a specific step in the care workflow?
11
Are the processes disclosed including experts used to develop tool?
Group 2 considered responses for each criteria and possible scoring methodologies. The consensus for this group was that the yes/no format was not appropriate for these criteria and a likert-type scaled metric would be needed. The group also noted that it would be important to be consistent about what scale is employed and the methods used to score criteria. This consistency will allow for establishing benchmarks based on criteria that are actually comparable. The group recommended a 1-4/5 scale and a process that would require a minimum score over a series of criteria.
The group called attention to the need to consider language and specific wording for different types of DSTs. The language for tools that include treatment options, other types of clinical information or possibly decision criteria for diagnostic or screening interventions is likely to differ to match the context of the criteria.
Summary and Next Steps
Our goal in this project is to take what we have learned to develop a user-friendly, patient-centered platform for creating and evaluating decision support tools. The excellent work done by IPDAS and others provides the scaffolding on which we are building a new, enhanced platform for DSTs. We will continue to involve external reviewers from a broad range of fields, including patients, advocates, educators and DST developers, to advise us as we move forward and evaluate criteria as we identify them.
We plan to publish a series of articles summarizing our work to date with recommendations for best practices for including and assessing person-centered criteria in decision support tools.
We welcome your comments and observations on this important topic and will update this site as we progress.